
Introduction: His correlations say one thing, but Joshua Grubbs says another
The researcher who saddled humankind with “perceived pornography addiction” and claimed it somehow “functions very differently from other addictions,” has now turned his dexterity to porn-induced ED. Joshua Grubbs’s new paper claims there’s no epidemic of youthful ED, boldly concluding its abstract with:
In conjunction with prior literature, we conclude that there is little or no evidence of an association between mere pornography use and ED.
This two-part assertion is disturbingly inaccurate:
- In reality, this new Grubbs study actually found that both problematic porn use (porn addiction) and higher levels of porn use were related to poorer erectile functioning in all 3 samples.
- As for “prior literature,” about 40 studies link porn use or porn addiction to sexual problems and lower arousal to sexual stimuli. In fact, the first 7 studies in that list demonstrate causation, as participants eliminated porn use and healed chronic sexual dysfunctions.
Equally disturbing is the fact that this paper:
- largely excluded men with severe erectile dysfunction
- excluded sexually inactive men, and
- excluded virgins.
In short, most of the young men who constitute the “ED epidemic” (which these authors deny) were omitted from this study. It’s easier to claim you have established that porn use isn’t associated with an ED epidemic, if you refuse to study those who are suffering so severely from porn-induced ED that they aren’t having sex!
As RebootNation founder Gabe Deem said about a similar study: “Using men with healthy erections to study the links between porn and ED is akin to using cancer-free subjects to study the links between smoking and lung cancer.” (Gabe recovered from severe PIED, and now helps other men porn-induced sexual problems.)
Even though this Grubbs-penned study found correlations between poorer sexual functioning and both porn addiction and porn use (while excluding sexually inactive men and thus many men with ED), the paper reads as if it has completely debunked porn-induced ED (PIED). This maneuver comes as no surprise to those who have followed the earlier dubious claims of Dr. Grubbs in relation to his “perceived pornography addiction” campaign.
Note: While the study lists both Joshua Grubbs and Mateusz Gola as authors, Grubbs was responsible for “Acquisition of Data,” “Analysis and Interpretation of Data,” and “Drafting the Article.” Gola jumped in after the fact, helping only with “Revising It for Intellectual Content.” This is Josh Grubbs’s baby.
Let’s examine the problems in the methodology and reported findings:
Red Flag: The 3 groups of sexually active men reported good sexual functioning
Note the average age of each group. Sample 3 contains the age range most affected by porn as it’s rare for 19-year olds (sample 1) to develop PIED, while men in their late 40s to early 60s (sample 2) didn’t grow up using streaming internet porn. 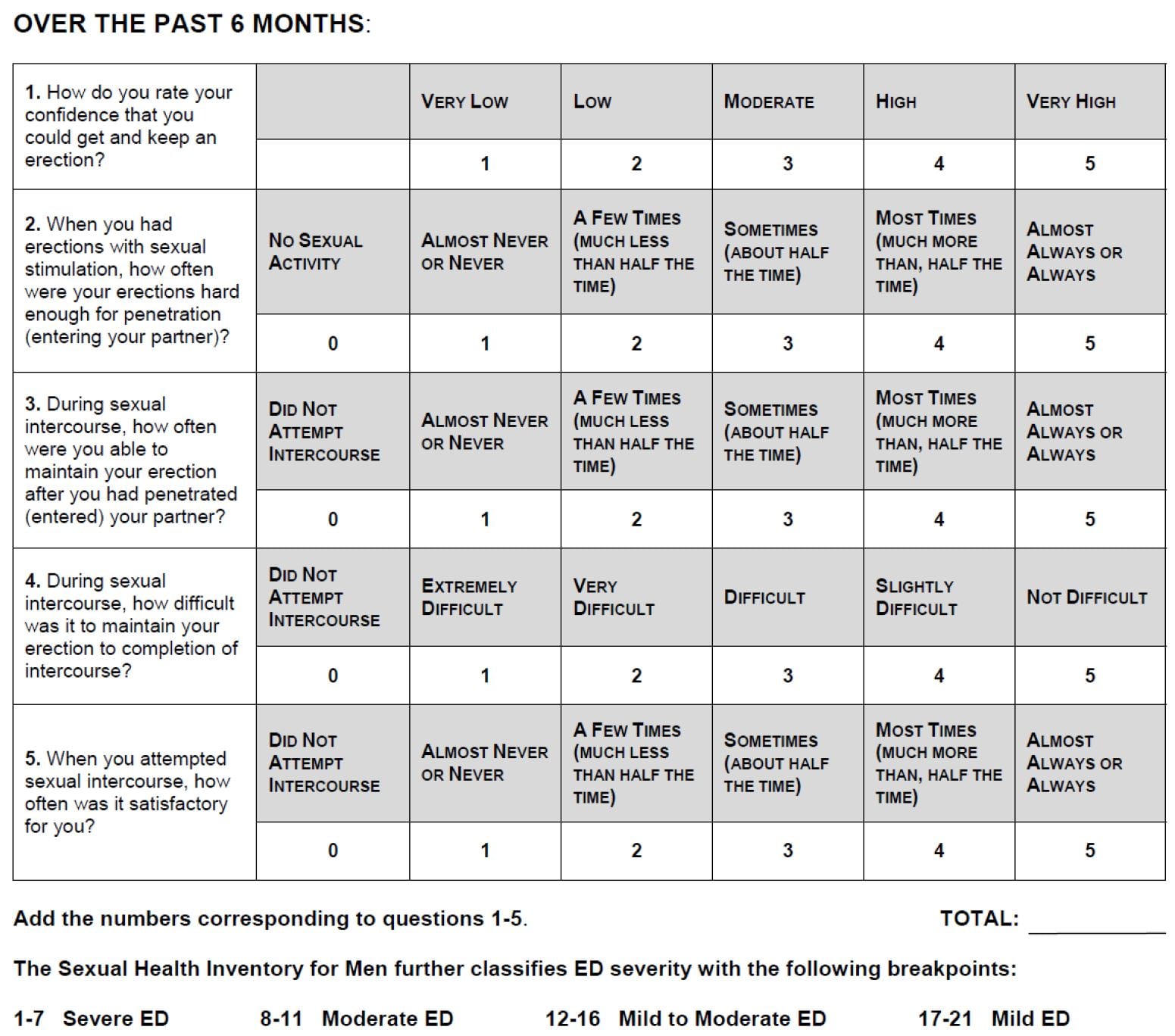
- Sample 1: Psychology students: average age 19.8 (N=147)
- Sample 2: Online survey: average age 46.5 (N=297)
- Sample 3: Online survey: average age 33.5 (N=433)
As the study reported, all 3 groups scored fairly high on erectile functioning (using the IIEF-5) :
In 3 samples of sexually active men who also consume pornography, we found very high levels of erectile functioning. (emphasis supplied)
Again, this constitutes a huge confound as the study omitted virgins, sexually inactive men, and most anyone with severe ED: the very men who have the most porn-related sexual problems. The men excluded from the study represent a significant portion of the population, as there has been a tremendous rise in sexually inactive young men and men men under 40 with ED or problematic low libido.
It’s important to note that the IIEF-5 (pictured above) is intended to assess only men who are engaging in sexual intercourse (sexually active men). In fact, a sexual medicine physician said the IIEF is only validated with respect to men who have had sex in the last 4 weeks.
If complete porn-induced ED is a porn user’s current destination, many recognizable steps often preceded it, sometimes by years. As such, many porn-related sexual problems (and the men who have them), would be ineligible for assessment using the IIEF-5. Here are common issues reported on porn recovery forums:
- Difficulty reaching orgasm with a partner (delayed ejaculation)
- Needing to recall porn to maintain erection or interest in sexual partner
- Greater sexual excitement using porn than with a partner
- Earlier genres of porn are no longer “exciting”
- Declining sexual arousal with a sexual partner(s)
- Can’t maintain erection or ejaculate with oral sex
This grim reality is supported by at least 7 studies demonstrating porn use apparently causing an array of sexual dysfunctions. Three of the six studies involved men who recovered from porn-induced anorgasmia and low libido, rather than ED. The other two studies contained a mix of patients who healed porn-induced delayed ejaculation and PIED. In addition, a study on treatment-seeking men who compulsively masturbated to porn reported that 71% of them had sexual problems, with 33% reporting delayed ejaculation.
Bottom line: In addition to likely omitting many (or even most) of the young men who constitute the “ED epidemic,” the study did not catch other porn-related sexual problems reported in the literature and by many chronic porn users.
Contrary to Grubbs’s study analysis (and his tweets), both porn addiction and higher levels of porn use were related to poorer erectile functioning
Tips for understanding the numbers in the study’s tables:
Zero means no correlation between two variables; 1.00 means a complete correlation between two variables. The bigger the number the stronger the correlation between the 2 variables. If a number has a minus sign, it means there’s a negative correlation between two things. (For example, there’s a negative correlation between exercise and heart disease. Thus, in normal language, exercise reduces the chances of heart disease. In contrast, obesity has a positive correlation with heart disease.)
Part 1: Porn addiction and erectile functioning
The 4 questions Grubbs used to measure levels of problematic porn use (porn addiction) were:
- I believe I am addicted to Internet pornography
- I feel unable to stop my use of online pornography
- Even when I do not want to view pornography online, I feel drawn to it
- I have put off things I needed to do in order to view pornography
A reader of the paper’s Introduction or Discussion sections would likely miss the fact, but both levels of porn use and levels of problematic porn use (porn addiction) were related to lower scores on IIEF-5 (the International Index of Erectile Function), which indicates reduced erectile functioning. Yet, even the authors do admit that porn addiction was related to poorer erectile functioning:
Similarly, there were consistent negative relationships between erectile functioning and problematic pornography use in all 3 samples, although this relationship was of only small to moderate magnitude (r = –0.20 to –0.33) and did not maintain statistical significance in sample 1 after application of the Holm correction.
Remember, a negative signs means lower scores on the IIEF, which means poorer erectile functioning. The results reveal that even in subjects with relatively healthy erectile functioning, porn addiction was significantly related to poorer erections.
Wait a minute you ask, how dare I say significantly related? Doesn’t the the study excerpt above confidently declare that the relationship (–0.20 to –0.33) was only “small to moderate,” meaning it’s no big deal?
As we will explore in greater detail below, Grubb’s use of descriptors varies remarkably, depending upon which Grubbs study you read. If the Grubbs study is about porn use causing ED, then the above numbers represent a meager correlation, tossed aside in his spin-laden write-up.
However, if it’s Grubbs’s most famous study (“Transgression as Addiction: Religiosity and Moral Disapproval as Predictors of Perceived Addiction to Pornography“), where he proclaimed that being religious was the real cause of “porn addiction,” then numbers smaller than these constitute a “robust relationship.” In fact, Grubbs’s “robust” correlation between religiosity and “perceived pornography addiction” was only 0.30! Yet he audaciously used it to usher in a completely new, and questionable, model of porn addiction. The tables, correlations and details referred to here are found in this section of a longer YBOP analysis.
In the current ED study, it’s vital to note that the strongest correlation between porn addiction and poorer erections (–0.33) occurred in Grubbs’s largest sample. This was the only sample of an average age most likely to report porn induced ED: sample 3, average age: 33.5 (433 subjects).
Part 2: Pornography use and erectile functioning
While the paper consistently downplays the correlations between higher pornography use and poorer erections, correlations were reported in all 3 groups – especially for sample 3, which was the most relevant sample as just explained. Excerpt from study:
However, with the exception of sample 3, there was little evidence of a link between pornography use itself and erectile functioning. In samples 1 and 2, the links between pornography use and erectile functioning were consistently weak and insignificant
Below are the 3 groups, with their average daily minutes of porn viewing and the correlations between erectile functioning amount of use (a negative sign means poorer erections linked to greater porn use):
- Sample 1 (147 men): average age 19.8 – Averaged 22 minutes of porn/day. (–0.18)
- Sample 2 (297 men): average age 46.5 – Averaged 13 minutes of porn/day. (–0.05)
- Sample 3 (433 men): average age 33.5 – Averaged 45 minutes of porn/day. (–0.37)
Fairly straightforward results: the sample that used the most porn (#3) had the strongest correlation between greater porn use and poorer erections, while the group that use the least (#2) had the weakest correlation between greater porn use and poorer erections. Why didn’t Grubbs emphasize this pattern in his write-up, instead of using statistical manipulations to try to make it disappear?
To summarize:
- Sample #1: Average age 19.8 – Note that 19-year old porn users rarely report chronic porn-induced (especially when only using 22 minutes a day). The vast majority of porn-induced ED recovery stories YBOP has gathered are by men aged 20-40. It generally takes time to develop PIED.
- Sample #2: Average age 46.5 – They averaged only 13 minutes per day! With a standard deviation of 15.3 years, some portion of these men were fifty-something. These older men did not start out using internet porn during adolescence (making them less vulnerable to conditioning their sexual arousal solely to internet porn). Indeed, just as Grubbs found, the sexual health of slightly older men has always been better and more resilient over all, than users who began using digital porn during adolescence (such as those with an average age of 33 in sample 3).
- Sample #3: Average age 33.5 – As already mentioned, sample 3 was the largest sample and averaged higher levels of porn use. Most importantly, this age range is the most likely to report PIED. Not surprisingly, sample 3 had the strongest correlation between higher levels of porn use and poorer erectile functioning (–0.37).
Considering the above links between poorer erections and both greater porn use and porn addiction, it’s shocking how this Grubbs paper reads as if widespread internet porn cannot be related to the documented rise in ED in men under 40. Also, why did Grubbs disregard the robust correlations in the age group most affected by PIED and who reported the greatest porn use? Was he unaware of the age ranges most affected by porn induced sexual problems?
Put simply, if this study had only addressed sample #3 (which was apparently the first sample Grubbs gathered), Grubbs would have been obliged (we hope) to acknowledge porn’s relationship to sexual dysfunction. Instead, two samples outside the target age range, were added after the baseline scores for sample #3 were gathered. This watered down the initial and most relevant findings (sample #3).
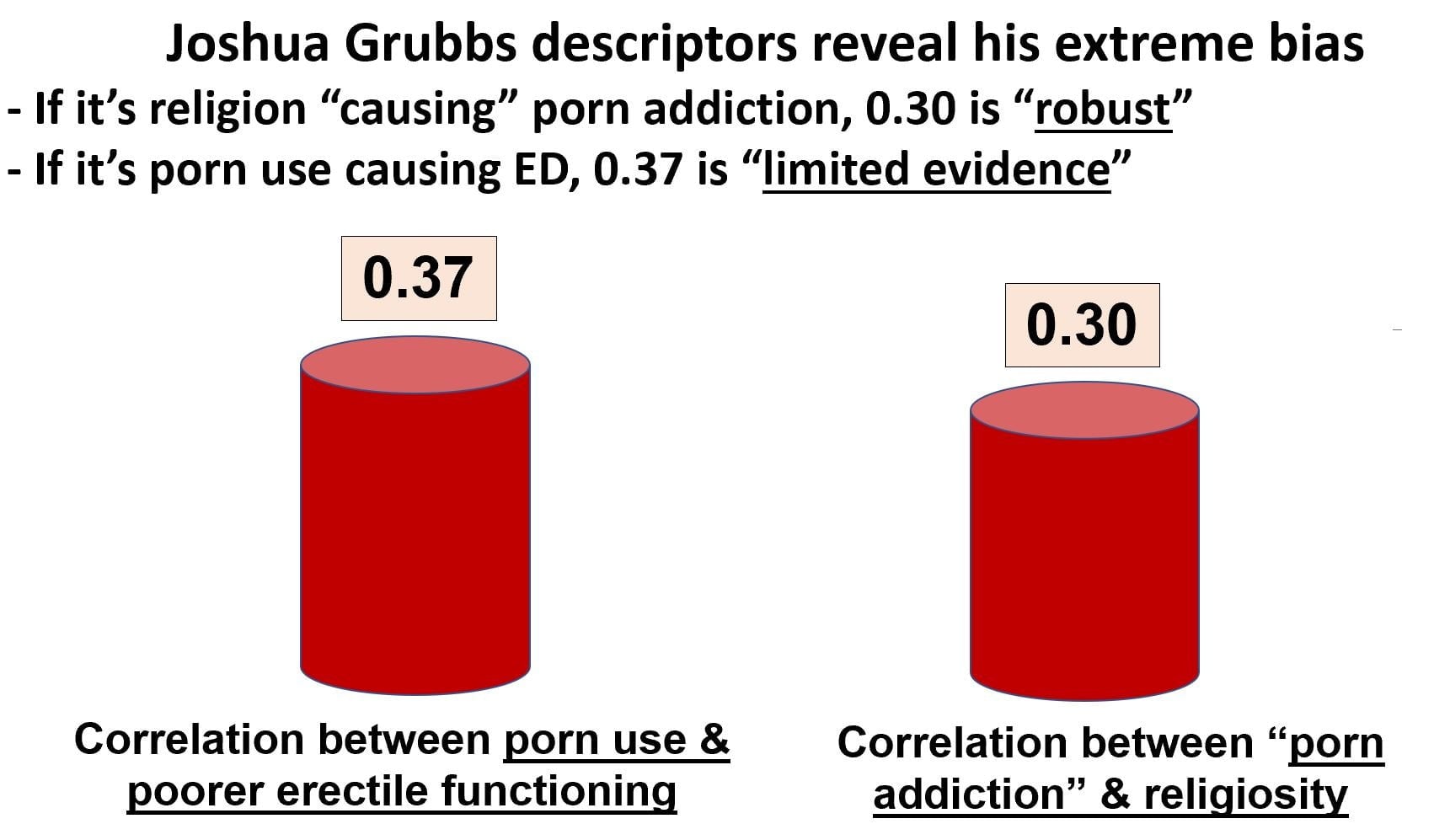
Grubbs: If it’s religion causing porn addiction, 0.30 is “robust.” If it’s porn causing ED, 0.37 is “limited evidence.”
As mentioned above, Grubbs has in the past unhesitatingly used weaker correlations than those reported in the current ED study to make very strong and questionable claims in his most highly publicized studies. Grubbs’s claim to fame is his series of “perceived porn addiction” studies, which spawned the scientifically inadequately supported meme that “religion causes porn addiction.” Too intricate to unpack here, YBOP (and actual researchers) have dismantled Grubbs’s unsupported claims elsewhere: article 1, article 2, article 3.
However, before leaving this point, check out the data from Grubbs’s most widely cited paper: “Transgression as Addiction: Religiosity and Moral Disapproval as Predictors of Perceived Addiction to Pornography.” Table 2 below contains data from 2 separate samples. Highlighted below are the correlations between Grubbs’s porn use questionnaire, the CPUI-9 (#1), and Religiosity (#6).
Here’s something to keep in mind when reading all of Grubbs’s perceived-addiction studies: he re-labeled the total CPUI-9 score as “perceived pornography addiction” – even though it was not a perception-of-addiction test. This is confusing, yet highly strategic, as his studies and comments on social media read as if he assessed “belief in porn addiction,” although he did not. So when Grubbs states that religiosity is robustly related to “perceived porn addiction,” he really means that religiosity is merely related to total score on his CPUI-9, an unsound questionnaire that assesses neither actual porn addiction nor believing oneself to be a porn addict.

The correlations between total CPUI-9 scores and religiosity: Study 1: 0.25, Study 2: 0.35
- Average: 0.30
What did Dr. Grubbs say about the 0.30 relationship between “perceived pornography addiction” and religiosity? Why, he claimed it was “robust!”
Results from two studies in undergraduate samples (Study 1, N=331; Study 2, N=97) indicated that there was a robust positive relationship between religiosity and perceived addiction to pornography.
Grubbs considers 0.30 “robust” when it supports his artfully crafted meme that religious folks only “perceive” they are addicted to porn and no one else really has a problem with it.
In the current ED study, how has Grubbs described the correlations between greater porn use and poorer erections, including sample 3 – which had a larger correlation (0.37), than his “religion = porn addiction” study just described?
“Across the 3 samples, we found only very limited support for the notion that mere pornography use itself is related to diminished erectile functioning, which is inconsistent with another popular narrative claiming that such use is likely to drive sexual dysfunction.” (emphasis supplied)
In 2019, Grubbs considers 0.37 as “very limited support” for a link between porn use and poorer erectile functioning. Have Grubbs’s views on statistics evolved in the intervening 4 years or could it be something else?
We suspect bias, and now revisit the above table from Grubbs “Transgression as Addiction“ study to support our assertion. Above we highlighted the correlations between CPUI-9 scores (perceived porn addiction) and religiosity. Below we highlighted the correlations between CPUI-9 scores (perceived porn addiction) and “hours of porn use”:
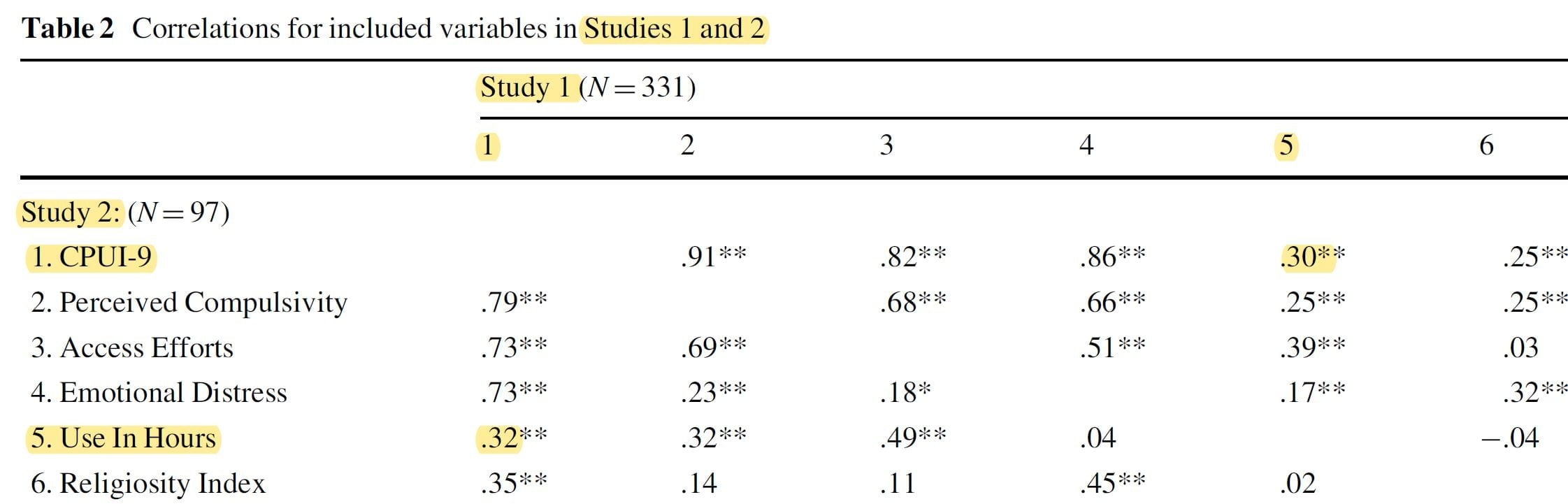
The correlations between total CPUI-9 scores (perceived porn addiction) and “hours of porn use”: Study 1: 0.30, Study 2: 0.32
- Average 0.31
Notice that CPUI-9 scores have a slightly stronger relationship to “hours of porn use” (0.31) than to religiosity (0.30). Put simply, hours of porn is a better predictor “perceived porn addiction” than is religiosity. It’s “porn overuse = porn addiction,” not “religiosity = porn addiction.” Even in Grubbs’s own work.
Yet Grubbs assures us that religiosity is “robustly related to perceived porn addiction” (CPUI-9 scores). If this is the case, then “hours of porn use” are evidently also “robustly related” to scores on the CPUI-9. But that’s not what you glean from reading the Grubbs’s analysis, or from his comments in the press or his Twitter feed.
Indeed, Grubbs sums up his campaign in this extraordinary biased 2016 Psychology Today article, where he falsely asserts that CPUI-9 scores (perceived porn addiction) are not related to the amount of porn used, but only related to religiosity:
Being labeled “porn addict” by a partner, or even by oneself, has nothing to do with the amount of porn a man views, says Joshua Grubbs, assistant professor of psychology at Bowling Green University. Instead, it has everything to do with religiosity…
… Grubbs calls it “perceived pornography addiction.” “It functions very differently from other addictions.” (emphasis supplied)
These are astonishing statements made in direct opposition to his findings. As the tables show, CPUI-9 scores (“perceived porn addiction”) were in fact more related to “hours of use” than to religiosity! Such unsupported assertions led YBOP to publish extensive critiques of Dr. Grubbs’s perceived porn addiction studies.
Now, we must do so again with this current ED paper, where he produced a write-up that dismisses significant correlations (especially in the most at-risk group), omits the numerous studies linking porn to sexual problems, and misrepresents the literature on sexual problems in young men. The picture this paper has painted matches neither his data nor the current state of the literature. Sadly, Grubbs even resorted to mischaracterizing his correlations on twitter:
In the Dr. Grubbs bizzaro-stats world view, 0.37 is not detectable (correlation between porn use & poorer erectile functioning), while 0.30 is robust (correlation between religiosity & perceived porn addiction).
Sample shell game?
To return to the matter of Grubbs’s samples, it’s common knowledge on porn recovery forums that the age group of men currently reporting the most porn-induced sexual problems hovers around late 20s and early 30s. In other words, of Grubbs’s three samples, the sample most suitable for investigating a possible phenomenon of porn-induced sexual dysfunction was sample 3.
Sample 3 (average age 33.5) is not only the closest sample to the ideal age group, but also by far the largest, and therefore most reliable, of his samples.
Interestingly, sample 3 was apparently the earliest of the samples Grubbs collected (spring of 2017). Predictably, sample 3 showed a robust correlation between impaired erectile health and porn use (0.37) and porn addiction (0.33) at baseline – even though many sexually inactive men had been (strategically?) excluded by use of the IIEF.
This raises awkward questions. Why didn’t Grubbs write up his results only about this sample 3, the most at-risk group? Had he done so, this would have been a very different paper…offering solid support for the existence of porn-induced erectile health problems (we would hope).
Was it because Grubbs didn’t like the robust correlations between poorer erectile health and both porn use and porn addiction, which his most relevant, most reliable sample revealed? Why did he obscure his most pertinent results by adding 2 more samples of men from less at-risk age groups?
Longitudinal group saw little change in erectile function, but problematic users may have dropped out
The study claims that in the longitudinal sample (#3) links between porn use/porn addiction didn’t have an impact on erectile functioning over 1 year’s time
In short, self-reported problematic use of pornography was not associated with changes in erectile functioning over a 1-year period, likely due to the lack of change in erectile functioning in the sample overall.
Let’s examine this finding. First, it’s important to know that of the 433 participants in group #3 at baseline, a mere 117 participants had complete data for the entire year (4 data points and 4 intervals). That’s a scant 27% of the original participants, on which Grubbs basis this claim.
Second, it appears likely that the subjects who used the most porn, and had the most problems (addiction), were the ones who tended to drop out of the study. Table 3 reveals a drop in average “hours of porn use” and porn addiction scores occurring with each successful check-in. Either all the men cut down on porn use and felt less addicted, or many of the heavier users with the worst problems dropped out. The latter seems most likely.
For both of these reasons we need to take this study’s longitudinal data with a boulder of salt.
Grubbs uses specious reasoning to suggest that “Moral incongruence”might explain poorer erectile functioning
Grubbs asserts that “Moral Incongruence” may play a role in ED, but he is playing games:
In addition, we note that in the 1 sample (sample 3) in which pornography use itself was related to diminished erectile functioning cross-sectionally, both self-reported problematic use and moral incongruenceregarding pornography use were similarly related to diminished erectile functioning, both of which in addition to the relationship between reported use and diminished erectile functioning. When these findings are considered along with the results from our other 2 samples demonstrating no clear relationship between pornography use and erectile functioning, we urge caution in placing credence on statements of pornography use itself as a causal mechanism in driving ED. (emphasis supplied)
MI (moral incongruence) is always correlated with porn addiction (Grubbs’s 4 questions listed earlier), because people with porn addiction usually want to stop due to negative consequences. Since MI is always related to porn addiction, and poorer erectile functioning always related to porn addiction, MI scores are related to poorer erectile functioning. So, Grubbs’s assertion is an artifact, not a meaningful correlation.
Note: Grubbs has been striving to convince the scientific community for 8 years that porn addiction is really nothing more than so-called “moral incongruence” (or religiosity). That is, disapproval of one’s own own compulsive porn use is the actual problem – not the porn use itself. His crusade rests on the unsupported premise that morally disapproving of one’s compulsive use is unique to porn addicts. However, this review of the literature points out the obvious. Addicts typically disapprove of their addictions. Here drug addicts cite moral reasons as core motivation for quitting:
Grubbs should ask himself, “Why isn’t there a ‘moral disapproval model’ of meth addiction, or gambling addiction, or cigarette addiction?” The ‘moral disapproval model of porn addiction’ is a red herring spawned by Grubbs himself. It’s created and supported by his own repetitive studies correlating moral disapproval with porn addiction (and those of his fan club), while he ignores dozens of other important variables that better explain problematic porn use (such as inability to quit despite negative consequences).
The reality is that 51 neurological studies show that porn addiction functions very much like other addictions. And even Grubbs’s own studies consistently reveal that “perceived pornography addiction” scores have a lot to do with the amount of porn a man views.
Josh Grubbs allies himself with radical pro-porn, anti-PIED propagandists Nicole Prause & David Ley (and becomes a member of realyourbrainonporn)
Dr. Grubbs appears to be closely allied with ardent pro-porners Dr. Nicole Prause and Dr. David Ley. All three often like and retweet each other comments, entering into jovial Twitter convos ridiculing harms associated with internet porn overuse. All three campaign against the concept of “porn addiction.” Ley and Grubbs have co-authored peer-reviewed papers, and Ley and Prause have vocally championed Grubbs’s “perceived addiction” studies since the first one appeared.
SHOCKING UPDATE: In 2019, Joshua Grubbs confirmed his agenda-driven bias when both formally joined allies Nicole Prause and David Ley in trying to silence YourBrainOnPorn.com. Grubbs and other pro-porn “experts” at www.realyourbrainonporn.com are engaging in illegal trademark infringement and squatting. The reader should know that RealYBOP twitter (with the apparent approval of its experts) is also engaging in defamation and harassment of Gary Wilson, Alexander Rhodes, Gabe Deem and NCOSE, Laila Mickelwait, Gail Dines, and anyone else who speaks out about porn’s harms. Prause (who runs RealYBOP twitter) appears to be quite cozy with the pornography industry, and uses RealYBOP twitter to promote the porn industry, defend PornHub (which hosted child porn and sex trafficking videos), and attack those who are promoting the petition to hold PornHub accountable. We believe that RealYBOP “experts” should be required to list their RealYBOP membership as a “conflict of interest” in their peer-reviewed publications.
So it’s no surprise that Ley and Prause adore this current Grubbs study (at least his write-up, if not the actual correlations). In this Twitter thread, Prause suggests, without sound basis, that the “moral disapproval” correlation might mean that erection troubles are really porn-induced….via shame. Grubbs seems to agree with his ally:
Ley and Prause are not objective observers. Both have engaged in multiple documented incidents of harassment and defamation as part of an ongoing “astroturf” campaign to persuade people that anyone who disagrees with their conclusions deserves to be defamed. Prause appears to be quite cozy with the pornography industry, as can be seen from this image of her (far right) on the red carpet of the X-Rated Critics Organization (XRCO) awards ceremony. According to Wikipedia “the XRCO Awards are given by the American X-Rated Critics Organization annually to people working in adult entertainment. It is the only adult industry awards show reserved exclusively for industry members.[1]“(emphasis supplied)
David Ley is not only involved with several of the preceding incidents, he has also published multiple articles attacking porn recovery forums and the concept of porn induced ED, disparaging men who run porn-recovery forums and using social media to harass men recovering from PIED. In a blatant financial conflict of interest, David Ley is being compensated by porn industry giant X-hamster to promote their websites and to convince users that porn addiction and sex addiction are myths! Specifically, David Ley and the newly formed Sexual Health Alliance (SHA) have partnered with a X-Hamster website (Strip-Chat). See “Stripchat aligns with Sexual Health Alliance to stroke your anxious porn-centric brain“. In addition, Ley makes money selling two books which deny sex and porn addiction (“The Myth of Sex Addiction,” 2012 and “Ethical Porn for Dicks,” 2016). Is that a conflict of interest? Pornhub is one of the four back-cover endorsements for the book on Amazon.com.
And now we have Josh Grubbs, who has co-authored journal articles with buddy David Ley, joining Ley in making fun of porn-induced ED:
This Grubbs tweet is from May, 2017 – over 18 months before he published his current paper “debunking” porn-induced ED. Bias anyone?
Nicole Prause continues to be obsessed with debunking PIED, having spent the last 5 years harassing and libeling young men who have recovered from porn-induced sexual dysfunctions and are trying to warn others. See documentation: Gabe Deem #1, Gabe Deem #2, Alexander Rhodes #1, Alexander Rhodes #2, Alexander Rhodes #3, Noah Church, Alexander Rhodes #4, Alexander Rhodes #5, Alexander Rhodes #6, Alexander Rhodes #7, Alexander Rhodes #8, Alexander Rhodes #9, Alexander Rhodes#10, Alex Rhodes#11, Gabe Deem & Alex Rhodes together#12, Alexander Rhodes#13, Alexander Rhodes #14, Gabe Deem#4, Alexander Rhodes #15.
In addition, Prause (with Ley’s help) has waged a 4-year war against this review involving 7 US Navy physicians and Gary Wilson (published in the journal Behavioral Sciences): Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (Park et al., 2016). (For much much more see: Prause’s efforts to have Behavioral Sciences review paper (Park et al., 2016) retracted.) Joshua Grubbs has recently joined Prause and Ley in this unprofessional and unethical campaign against Park et al. 2016 and MDPI, engaging in ad hominem attacks, falsehoods, and cyber-harassment.
First example: on February 16, 2019, a sexual medicine specialist presented a talk at the 21st Congress of the European Society for Sexual Medicine on the Internet’s impact on sexuality. A few slides describing porn-induced sexual problems, citing Park et al., 2016, were tweeted. The tweets caused Nicole Prause, David Ley, Joshua Grubbs and their allies to direct a Twitter-rage at Park et al., 2016. In this thread Grubbs joins Prause in her usual set of falsehoods and ad hominem attacks:

All of the above is empty defamation as revealed here. Notice that in all of the Prause, Ley, and Grubbs tweets they never provide a single example of the paper’s “fraud” or “false claims.” Only ad hominen attacks and falsehoods. Since Prause was one of the six reviewers of Park et al., you would think she could excerpt a section and explain how it constitutes “fraud.” Never happens….and never will because the paper contains no fraud and all Navy rules were complied with in its compilation.
Grubbs not only attacked Park et al. with Prause-like empty drivel, he also groundlessly attacked the parent journal MDPI (just as Prause has repeatedly done). A two-tweet smear from January, 2019:
Additional tweets smearing MDPI. This time in the guise of a “poll.”
Here he goes again, attacking MDPI:
The Grubbs attacks on MDPI and Park et al. started about the time he published the very paper critiqued on this page. Coincidence? Most unlikely. Grubbs has always worn his agenda on his sleeve – dismissing porn addiction, internet addiction, while asserting that almost all problems with porn arise from religious morality (recklessly leaving his readers with the false impression that atheists can use porn and not experience negative effects). Now he is upping his social media game to match that of his mentors – Prause & Ley…. for example:
He must make his mentors proud.
Empty claims that a PIED epidemic doesn’t exist
This paper claims several times that there’s not an epidemic of ED, and that porn use is not related to claimed epidemic of ED:
Despite evidence to the contrary, a number of advocacy and self-help groups persist in claiming that internet pornography use is driving an epidemic of erectile dysfunction (ED).
We’ll begin with the first words of the above excerpt: there is no persuasive “evidence to the contrary.” Let’s examine this purported contrary evidence.
1) Prause and Pfaus, 2015: Prause and Pfaus did not support its claims. See a formal critique by researcher Richard Isenberg, MD and a very extensive lay critique:
- In the same journal as the paper: Letter to the editor by Richard A. Isenberg MD (2015)
- Extensive lay critique: Nothing Adds Up in Dubious Study: Youthful Subjects’ ED Left Unexplained (2015)
Prause and Pfaus 2015 wasn’t a study on men with ED. It wasn’t a study at all. Instead, Prause claimed to have gathered data from four of her earlier studies, none of which addressed erectile dysfunction. It’s disturbing that this paper by Nicole Prause and Jim Pfaus passed peer-review as the data in their paper did not match the data in the underlying four studies on which the paper claimed to be based. The discrepancies are not minor gaps, but gaping holes that cannot be plugged. In addition, the paper made several claims that were false or not supported by their data. In addition, both Nicole Prause and Jim Pfaus made false statements to the media about their methodology and findings.
2) Landripet and Štulhofer, 2015 was designated as a “brief communication” by the journal that published it, and the two authors selected only certain data to share, while omitting other pertinent data. As with Prause and Pfaus, the journal later published a critique addressing the weaknesses of Landripet and Štulhofer: Comment on: Is Pornography Use Associated with Sexual Difficulties and Dysfunctions among Younger Heterosexual Men? by Gert Martin Hald, PhD
As for the claim that Landripet and Štulhofer, 2015 found no relationships between porn use and sexual problems, this is not true, as documented in both this YBOP critique and this review of the literature, co-authored by multiple Navy physicians. Furthermore, Landripet and Štulhofer’s paper omitted three significant correlations, which one of the authors had earlier presented at a European conference.
Equally importantly, in his write-up, why did Grubbs ignore the 27 peer-reviewed studies linking porn use/porn addiction to sexual problems and lower arousal – especially the 5 case studies where men healed problems by quitting porn?
Here’s a similar excerpt where he attempts to press home his same flawed talking point about the state of the literature:
In general, among sexually active pornography-using men, serious erectile problems seem rare, a finding that runs counter to a popular narrative suggesting that pornography use is driving an epidemic of ED.
In fact, as noted above, the 3 samples here were men who are sexually active and whose IIEF (sexual health) scores were pretty good. Put simply, this paper largely excluded men with ED, didn’t include sexually inactive men, and didn’t include virgins. Thus, many of the the men who constitute the “ED epidemic” (which these authors deny) were omitted from this study. And yet, even in this paper both porn addiction and higher levels of porn use were related to poorer erectile functioning. Why go to such pains to deny the truth?
The position of the “medical community”?
Citing nothing to support their assertion, Grubbs and his co-author mistakenly claim that the “medical community” has not conclusively found evidence of an epidemic of ED:
Moreover, given that the medical community has not conclusively found evidence of an increasing rate of ED in young men in recent years, the present work provides additional evidence against the notion that pornography use is driving an epidemic of ED.
The reality?
Historical ED rates: Erectile dysfunction was first assessed in 1940s when the Kinsey report concluded that the prevalence of ED was less than 1% in men younger than 30 years, less than 3% in those 30–45. While ED studies on young men are relatively sparse, this 2002 meta-analysis of 6 high-quality ED studies reported that 5 of the 6 reported ED rates for men under 40 of approximately 2%. The 6th study reported figures of 7-9%, but the question used could not be compared to the 5 other studies, and did not assess chronic erectile dysfunction as had the others. Instead it asked, “Did you have trouble maintaining or achieving an erection any time in the last year?”
At the end of 2006, free, streaming porn tube sites came on line and gained instant popularity. This changed the nature of porn consumption radically. For the first time in history, viewers could escalate with ease during a masturbation session without any wait. What happened to ED rates?
Ten studies since 2010: Ten studies published since 2010 reveal a tremendous rise in erectile dysfunction. This is documented in this lay article and in this peer-reviewed paper co-authored by 7 US Navy physicians – Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016). In the 10 studies, erectile dysfunction rates for men under 40 ranged from 14% to 37%, while rates for low libido ranged from 16% to 37%.
Other than the advent of streaming porn (2006) no variable related to youthful ED has appreciably changed in the last 10-20 years (smoking rates are down, drug use is steady, obesity rates in males 20-40 up only 4% since 1999 – see this study).
The recent jump in sexual problems coincides with the publication of over 35 studies linking porn use and “porn addiction” to sexual problems and lower arousal to sexual stimuli. In addition to the studies listed, this page contains articles and interviews involving over 150 experts (urology professors, urologists, psychiatrists, psychologists, sexologists, MDs) who acknowledge, and have successfully treated, porn-induced ED and porn-induced loss of sexual desire.
Current hours of porn use is just one of many variables that may predict porn-induced sexual dysfunctions
Additional variables likely also need to be investigated. This 2016 review highlighted the weakness in correlating only “current hours of use” to predict porn-induced sexual dysfunctions. The amount of porn currently viewed is likely just one of many variables related to the development of porn-induced ED. Others may include:
- Ratio of masturbation to porn versus masturbation without porn
- Ratio of sexual activity with a person versus masturbation to porn
- Gaps in partnered sex (where one relies only on porn)
- Virgin or not
- Total hours of use
- Years of continued use
- Age started using porn voluntarily
- Escalation to new genres
- Development of porn-induced fetishes (from escalating to new genres of porn)
- Level of novelty per session (i.e. compilation videos, multiple tabs)
- Addiction-related brain changes or not
- Presence of hypersexuality/porn addiction (which was robustly related in sample #3)
- It might also be fruitful to ask about edging, the harmful practice of masturbating to porn while avoiding climax.
The better way to research this phenomenon, is to remove the variable of internet porn use and observe the outcome, which was done in multiple case studies in which men removed internet porn use and healed. Such research suggests causation instead of correlations based on possibly faulty recall – and open to agenda-driven interpretations like those in the present study. YBOP has documented self-reports of a few thousand men who removed porn and recovered from chronic sexual dysfunctions.
Additional flaws, also present in earlier papers on the subject
Some of the following points come from this earlier critique of Prause and Pfaus 2015. The current paper suffers from most of the same flaws.
- Did not assess individuals complaining of erectile dysfunction
- Did not ask men to attempt masturbation without porn (the way to test for porn-induced ED)
- Did not have men remove porn to see if erectile functioning eventually improved (the only way to know if ED was porn-induced)
- Did not ask about years or porn use, age guys started using porn, type of porn, or escalation of use.
- Did not ask about delayed ejaculation or anorgasmia (precursors to PIED)
- Study only included men who were sexually active (which means they probably didn’t have full blown ED), which would exclude those with such severe ED that they are avoiding sex
- Study omitted virgins (including so called “porn virgins” – who can’t manage sex with real partners) and thus all who have not had sex in the last year.
Conclusion
A genuine investigation of porn use and sexual dysfunctions needs to ask subjects to eliminate digital porn use and assess any changes over the subsequent months.
Meanwhile, it is evident that the scientific community can do a more conscientious job of investigating the unfortunate phenomenon of young men in their prime struggling with unprecedented levels of sexual dysfunctions (which often heal simply by giving up today’s ubiquitous digital porn). Researchers can also do a far more responsible job of describing their findings and the state of the literature rather than misleading their readers.