Central Mechanisms of Erectile Dysfunction: What a Clinician May Want to Know
International Journal of Impotence Research (2003) 15, Suppl 2, S3–S6. doi:10.1038/sj.ijir.3900989
C G Stief1
1Medical School Hannover, Department of Urology, Hannover, Germany
Abstract
The interplay between peripheral and central mechanisms of erectile function are not fully elucidated although basic science is moving ahead in this area. It is important from a clinical point of view to understand these mechanisms so that we may begin to make further therapeutic advances in the treatment of erectile dysfunction (ED). It is now widely understood that central disinhibition plays a crucial role in the induction of erectile responses and this has led to the development of the central initiator, apomorphine SL (Ixense™) [apo SL]. Apo SL acts in the paraventricular nucleus of the hypothalamus as a dopamine receptor agonist. It works as a proerectile conditioner at this level to increase the responses of the erectile pathway following appropriate sexual stimulation. This unique central mode of action of apo SL has thus proved efficacious in approximately 70% of ED patients although persistence may be required to produce a robust effect for the maximum number of patients.
Introduction
Although the mechanisms underlying erectile function are not fully understood, advances have been made regarding the interplay of central and peripheral mechanisms. Understanding these mechanisms through basic science is crucial if the search for effective medicines to treat sexual function disorders such as erectile dysfunction (ED) is to be successful. The development of a class of drugs known as central initiators of erection such as apo SL has provided a useful addition to the armamentarium of the urologist, yet further work may assist in the identification of other potentially effective points of intervention in the erectile function pathway.
Central control of erectile function
Central mechanisms, both supraspinal and spinal, play an important role in erectile function (Figure 1). A ‘natural’ erection is initiated in the brain as a result of sexual stimuli which require processing and integration in order to initiate an appropriate erectile response. Visual, olfactory, tactile and imaginative stimuli from the occipital lobe, rhinencephalon, thalamus and limbic system, respectively, are integrated and processed into erectile responses in two small hypothalamic nuclei, the paraventricular nucleus (PVN) and medial preoptic area (MPOA).
Figure 1.
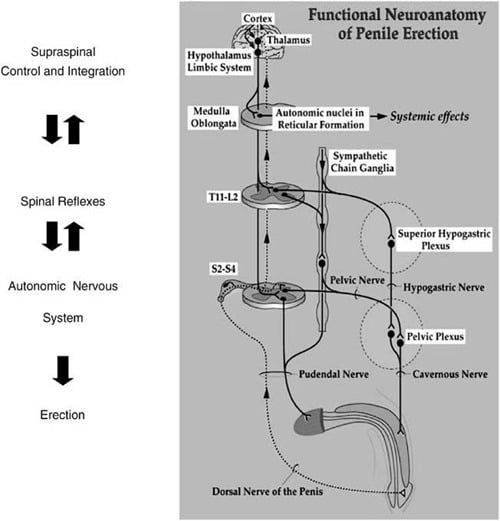
The role of the MPOA is to recognise sensory stimuli from the higher brain centres and integrate them with sexual motivation and copulatory motor programmes.1 The MPOA is also involved in maternal behaviour,2 thermoregulation3 and thirst.4 The PVN plays a key role in the erectile response, and pharmacological or electrical stimulation of this small hypothalamic nuclei results in seminal discharge in unanaesthetised rats5 and erection and ejaculation in anaesthetised rats.6 Dopaminergic neurones belonging to the incertohypothalamic dopamine system are the main components of the PVN. These dopaminergic neurones impinge on oxytocin containing neurones.7
Spinal processing of the erectile response
Neurones from the PVN run down through the mid-brain, and at this level the nucleus paragigantocellularis can interrupt proerectile signals from higher brain regions if it becomes inappropriate to have an erectile response.8,9 This is mediated through a serotinergic mechanism although the receptor subtypes involved are not fully elucidated.8 Once through the mid-brain, the erectile signals pass along the spinal cord to the periphery. In addition to transmitting neural signals, the spinal cord has an integrative role processing signals from peripheral and higher central regions. There are two main sites of integration for erectile function in the spinal cord, the sacral erection spinal centre from S2 to S4 and a thoracic-based centre from T11 to L2.10 Erectile signals leave the CNS at these two centres, and the information is then transferred through autonomic neurones to the periphery.
Peripheral neurotransmitters
There are a number of peripheral neurotransmitters implicated in the control of erections. Parasympathetic nitric oxide (colocalised with acetylcholine) innervation causes relaxation and results in erection,10 whereas noradrenergic sympathetic innervation results in detumescence.11 Other neurotransmitters involved in control of erectile function include nitric oxide and vasoactive interstitial peptide (VIP). The crucial peripheral event in the induction of erection is the relaxation of smooth muscle cells in the wall of the corpus cavernosum. This action is initiated in response to nitric oxide causing the rise of intracellular second messengers such as cAMP and cGMP, eventually resulting in calcium efflux from the cells and relaxation.12
Role of central dopamine in erectile function
There are a number of central neurotransmitters that are also involved in the initiation of erection; one such crucial neurotransmitter is dopamine. Dopamine is the main transmitter within the PVN,5 which, as discussed above, plays an important role in the central control of erection. Dopamine receptors are divided into two main families: D1- and D2-like receptors which are in turn subdivided from D1 to D5. Apo SL has a higher affinity for D2-like receptors13 that are thought to be the main site for the induction of erections in the PVN.14 Apo SL is therefore postulated to increase erectile responses by acting as a conditioner in the PVN, increasing the response to sexual stimuli resulting in enhanced erections induced in the periphery.15
Clinical efficacy of apo SL
The following question remains, how does this unique central mechanism of action and the basic science outlined above translate into clinical practice? Evidence for the postulated role for apo SL in the induction of erections has been accumulated during a number of clinical trials. More than 5000 men worldwide have been involved in these trials, receiving over 120 000 doses.16 These patients have represented a broad spectrum of ED patients. Men with concomitant disorders such as benign prostatic hyperplasia, coronary artery disease and diabetes have been included.16 Additionally, men with varying severities of ED, mild, moderate and severe, as assessed using the International Index of Erectile Function (IIEF) have been enrolled in the clinical trial programme. The primary end point in these clinical trials was the percentage of attempts resulting in an erection sufficiently firm enough for intercourse. The secondary end points were the percentage attempts at intercourse and partner satisfaction, both of which are highly clinically relevant. Assessment procedures utilised patient diaries and rating scales such as the IIEF.17
Apo SL has proved to be efficacious in ED, particularly in patients with mild-to-moderate ED.16 Approximately two-thirds of patients (Figure 2) will have a positive erectile response within the first 20 min of taking the drug although some patients will require longer (Figure 3).16 The efficacy of apo SL improves with repeat dosing; therefore, at least four doses are required to achieve intercourse. After four attempts, a robust response, with a two-fold increase in the percentage of erections firm enough for intercourse compared to placebo, can be expected with at least 70% of patients responding (Figure 4).18
Summary
Central disinhibition plays a key role in the induction of erection. There are a number of central structures implicated from higher cortical centres to hypothalamic nuclei, particularly the PVN. Stimulation of the D2-like receptors in the PVN has a proerectile effect. It is this stimulation via the D2 agonist apo SL that results in its clinical efficacy for men with ED.
The clinical efficacy of apo SL has been clearly demonstrated during double-blind crossover clinical trials in over 5000 men with varying degrees of ED from mild to severe. These studies have demonstrated a two-fold increase in the percentage of erections firm enough for intercourse compared to placebo and that apo SL is particularly effective in men with mild-to-moderate ED. The rapid onset of action of apo SL, occurring within 20 min for most patients could help men with ED improve spontaneity in their sexual relationships. The effectiveness of apo SL increases with sequential dosing for patients who sustain the treatment beyond four doses. This treatment regimen offers patients the opportunity of achieving satisfactory sexual performance.
References
1. McKenna KE. Central control of penile erection. Int J Impot Res 1998; 10(Suppl 1): S25–S34. | Article | PubMed |
2. Numan M. Neural basis of maternal behavior in the rat. Psychoneuroendocrinology 1988; 13: 47–62. | PubMed |
3. Kanosue K, Zhang YH, Yanase-Fujiwara M, Hosono T. Hypothalamic network for thermoregulatory shivering. Am J Physiol 1994; 267: R275–R282. | PubMed |
4. Bourque CW, Oliet SH, Richard D. Osmoreceptors, osmoreception, and osmoregulation. Front Neuroendocrinol 1994; 15: 231–274. | Article | PubMed | ISI | ChemPort |
5. Eaton RC et al. D2 receptors in the paraventricular nucleus regulate genital responses and copulation in male rats. Pharmacol Biochem Behav 1991; 39: 177–181. | Article | PubMed | ISI | ChemPort |
6. Chen KK, Chan SH, Chang LS, Chan JY. Participation of paraventricular nucleus of hypothalamus in central regulation of penile erection in the rat. J Urol 1997; 158: 238–244. | Article | PubMed | ISI | ChemPort |
7. Buijs RM, Geffard M, Pool CW, Hoorneman EM. The dopaminergic innervation of the supraoptic and paraventricular nucleus. A light and electron microscopical study. Brain Res 1984; 323: 65–72. | PubMed |
8. Marson L, McKenna KE. The identification of a brainstem site controlling spinal sexual reflexes in male rats. Brain Res 1990; 515: 303–308. | Article | PubMed | ISI | ChemPort |
9. Marson L, McKenna KE. A role for 5-hydroxytryptamine in descending inhibition of spinal sexual reflexes. Exp Brain Res 1992; 88: 313–320. | Article | PubMed | ISI | ChemPort |
10. Giuliano FA, Rampin O, Benoit G, Jardin A. Neural control of penile erection. Urol Clin North Am 1995; 22: 747–766. | PubMed | ISI | ChemPort |
11. Andersson KE, Hedlund P, Alm P. Sympathetic pathways and adrenergic innervation of the penis. Int J Impot Res 2000; 12: S5–S12. | Article | PubMed | ISI |
12. Wagner G, Mulhall J. Pathophysiology and diagnosis of male erectile dysfunction. BJU Int 2001; 88(Suppl 3): 3–10. | Article | PubMed |
13. Argiolas A, Hedlund H. The pharmacology and clinical pharmacokinetics of apomorphine SL. BJU Int 2001; 88(Suppl 3): 18–21. | Article | PubMed |
14. Chen KK, Chan JY, Chang LS. Dopaminergic neurotransmission at the paraventricular nucleus of hypothalamus in central regulation of penile erection in the rat. J Urol 1999; 162: 237–242. | Article | PubMed | ChemPort |
15. Rampin O. Mode of action of a new oral treatment for erectile dysfunction: apomorphine SL. BJU Int 2001; 88(Suppl 3): 22–24. | Article | PubMed |
16. Mirone VG, Stief CG. Efficacy of apomorphine SL in erectile dysfunction. BJU Int 2001; 88(Suppl 3); 25–29. | Article | PubMed |
17. Altwein JE, Keuler FU. Oral treatment of erectile dysfunction with apomorphine SL. Urol Int 2001; 67: 257–263. | Article | PubMed |
18. Heaton JP, Dean J, Sleep DJ. Sequential administration enhances the effect of apomorphine SL in men with erectile dysfunction. Int J Impot Res 2002; 14: 61–64. | Article |
19. Gerstenberg T, Hedlund H In: Graugaard C, Hertoft P, Møhl B (eds.). Hjerne & Seksualitet: Aspekter af Teori & klinik. Munksgaard, 1997